
| Human Breast Milk Biological Profile | |
|---|---|
| Evolutionary Origin | Synapsid Ancestors (~200 Million Years Ago) |
| Caloric Distribution | 50% Fat, 40% Carbs, 6% Protein |
| Average Caloric Density | 20 kcal per ounce |
| Osmolarity | 286 mOsm/L |
| Dominant Carbohydrate | Lactose (67 to 70 g/L) |
| Primary Whey Protein | Alpha-lactalbumin |
| Whey to Casein Ratio | 60 to 40 |
| Major Immunoglobulin | Secretory IgA (sIgA) |
| Target Intestinal Bacteria | Bifidobacterium longum subspecies infantis |
| Primary Genetic Modifiers | FUT2 (Secretor) and FUT3 (Lewis) |
| Tumoricidal Complex | HAMLET Complex |
| Stem Cell Type | Pluripotent-like hBmSCs |
| Circadian Sleep Regulator | Melatonin and Tryptophan |
| Official Health Guidelines | WHO Breastfeeding Guidelines |
| Biochemical Research Data | National Institutes of Health |
Human breast milk (HBM) is an evolutionary masterpiece, functioning as a highly conserved, incredibly dynamic biological fluid uniquely adapted to completely meet the precise metabolic, immunological, and developmental requirements of the human neonate. Far exceeding the traditional paradigm of mere somatic nutrition, HBM operates effectively as a living tissue and a sophisticated, bidirectional communication system deeply bridging maternal physiology and infant development. It brilliantly provides a highly bioavailable matrix of macronutrients and micronutrients, alongside an extensive, dense array of immunoglobulins, pluripotent stem cells, and highly bioactive molecules such as microRNAs (miRNAs) and human milk oligosaccharides (HMOs).
The evolutionary origin of mammalian lactation dates back over 200 million years to early synapsid ancestors, where primitive glandular secretions originally functioned to keep porous, parchment-like eggs moist before gradually evolving into complex, highly specialized nutrient delivery systems. In humans, this exact composition became exquisitely species-specific, reflecting the completely distinct evolutionary priority of the human species: massive and extremely rapid neurodevelopment, coupled with complex immunological programming, rather than the rapid somatic and musculo-skeletal hypertrophy seen in herd animals. This vital distinction separates human milk fundamentally from the milk of other mammals, such as bovines and caprines, which are biologically optimized for entirely different physiological trajectories.
This comprehensive report deeply explores the profound biochemistry, endocrinology, and cellular biology of human breast milk. We will rigorously analyze its anatomical formation, its exact macro-molecular architecture, the intricate genetic determinism of its oligosaccharides, and its profound, life-saving divergence from commercial substitute infant nutrition sources.
1. Mammogenesis and Structural Preparation
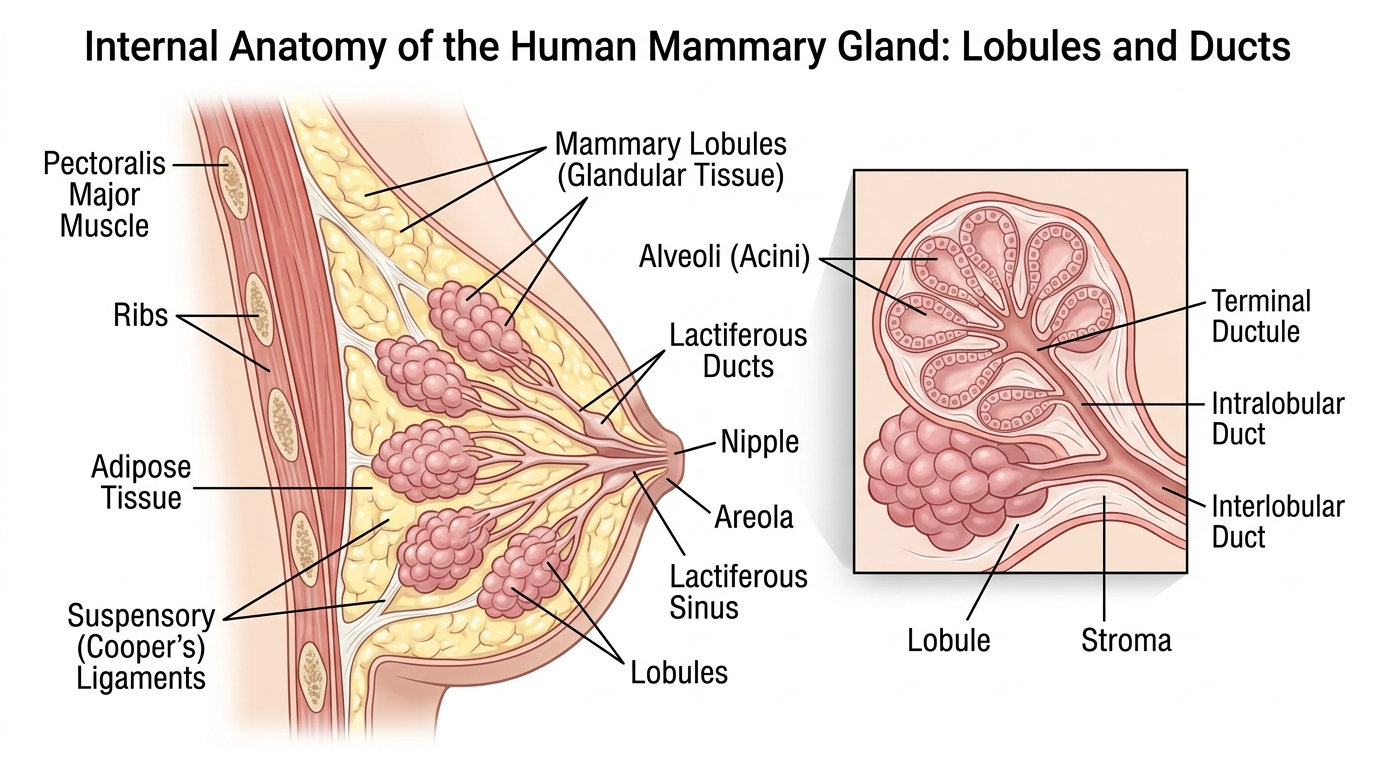
The biological preparation for, and subsequent execution of, milk synthesis and secretion is strictly governed by a highly orchestrated cascade of endocrine shifts. The foundation for lactation is definitively established well before parturition. During pregnancy, the maternal mammary glands undergo significant structural proliferation and differentiation completely under the synergistic influence of elevated circulating hormones, primarily estrogen, progesterone, prolactin, and human chorionic gonadotropin (hCG). Estrogen primarily facilitates the extensive branching, arborization, and elongation of the complex mammary ductal network.
Concurrently, progesterone makes crucial, mandatory contributions to alveologenesis, actively driving the genesis of the alveoli, the tiny, sac-like structures where milk is actually physically synthesized. This synergistic hormonal action brilliantly culminates in the formation of type III lobules, which are deeply characterized by highly abundant epithelial cells and active secretory acini. Furthermore, the external anatomy of the breast visibly alters to flawlessly accommodate feeding: the areolas become larger, and the Montgomery glands (small sebaceous glands on the areola) rapidly hypertrophy to selectively secrete vital antimicrobial oils that thoroughly lubricate and protect the sensitive nipple tissue during rigorous infant suckling. During late pregnancy, the hypertrophic alveoli undergo partial atrophy, a structural adjustment that carefully creates the necessary physical space within the lumen for colostrum to accumulate in preparation for birth.
2. Secretory Differentiation and Activation (Lactogenesis I & II)
Lactogenesis Stage I initiates approximately during the 16th week of gestation and persists until a few days immediately postpartum. During this initial phase, the mammary epithelial cells actively differentiate into a fully functional secretory state. The breasts begin safely synthesizing colostrum, a highly concentrated, very low-volume biological fluid massively enriched with powerful immunoglobulins, lactoferrin, and essential developmental growth factors. However, despite the presence of highly elevated systemic prolactin levels, which average between 100 to 300 μg/L in the maternal plasma at term, the actual secretion of large volumes of fluid milk is potently and completely inhibited by the massive concentrations of placental progesterone and estrogen circulating during pregnancy.
Stage II lactogenesis is triggered precisely by the physical expulsion of the placenta following childbirth. The removal of the placenta rapidly results in a precipitous, massive decline in plasma progesterone and estrogen concentrations. The sudden withdrawal of this steroidal inhibition un-suppresses the action of prolactin, allowing it to act directly and forcefully on the prolactin receptors situated securely on the mammary epithelial cells. By 4 to 5 days postpartum, the transition of the acinar epithelium from a pre-secretory to a fully secretory state is complete. A sharp escalation in citrate concentration occurs, serving as a highly reliable biochemical marker of Stage II lactogenesis, functioning alongside a distinct peak in plasma α-lactalbumin levels.
3. Galactopoiesis and Autocrine Regulation
Galactopoiesis, or Stage III lactogenesis, refers exactly to the ongoing, long-term maintenance of established milk production. While the initial onset of milk synthesis relies heavily on systemic endocrine shifts, its prolonged maintenance is primarily governed by highly localized autocrine control, dictated strictly by the physiological principle of biological supply and demand. The continuous synthesis, robust secretion, and delivery of milk rely entirely on the synergistic action of two primary hormones perfectly released in response to infant suckling or mechanical expression.
When the infant suckles, sensory nerve fibers rapidly transmit impulses through the mesencephalon to the hypothalamus, triggering the anterior pituitary gland to release prolactin into the bloodstream in a highly pulsatile manner to drive the continuous, de novo synthesis of milk. Concurrently, sensory impulses trigger the posterior pituitary gland to synthesize and release oxytocin. Oxytocin functions as an octapeptide hormone that binds to specific receptors located exactly on the myoepithelial cells that intricately envelop the alveoli, causing them to contract vigorously and physically propel the stored milk out of the alveoli in a phenomenon known as the milk-ejection reflex or let-down. Crucially, galactopoiesis is maintained by a local feedback mechanism governed by a specific whey protein known as the Feedback Inhibitor of Lactation (FIL). If milk is not effectively removed from the breast, the concentration of FIL accumulates heavily within the alveoli, where it exerts potent negative feedback to instantly cease further milk synthesis, safely protecting the fragile glandular tissue from dangerous mechanical engorgement.
4. Post-Lactation Involution
When the infant is eventually entirely weaned and regular milk removal permanently ceases, the mammary gland undergoes a highly programmed process of involution. The definitive cessation of lactation is strongly characterized by specific hormonal and morphological signals that safely return the breast to a non-secretory resting state.
A significant, measurable decrease in glucocorticoid hormones (dropping rapidly from 34 to 14 nM within just three days after the end of lactation) is absolutely required for breast involution and the programmed apoptosis of the excess secretory epithelial cells. Concurrently, maternal serum insulin levels increase significantly relative to the lactation period, and serum Insulin-like Growth Factor I (IGF-I) levels increase substantially exactly 21 days after the end of lactation, successfully mediating deep tissue remodeling and the total return to baseline glandular architecture.
5. Physiological Production Volumes and Infant Consumption
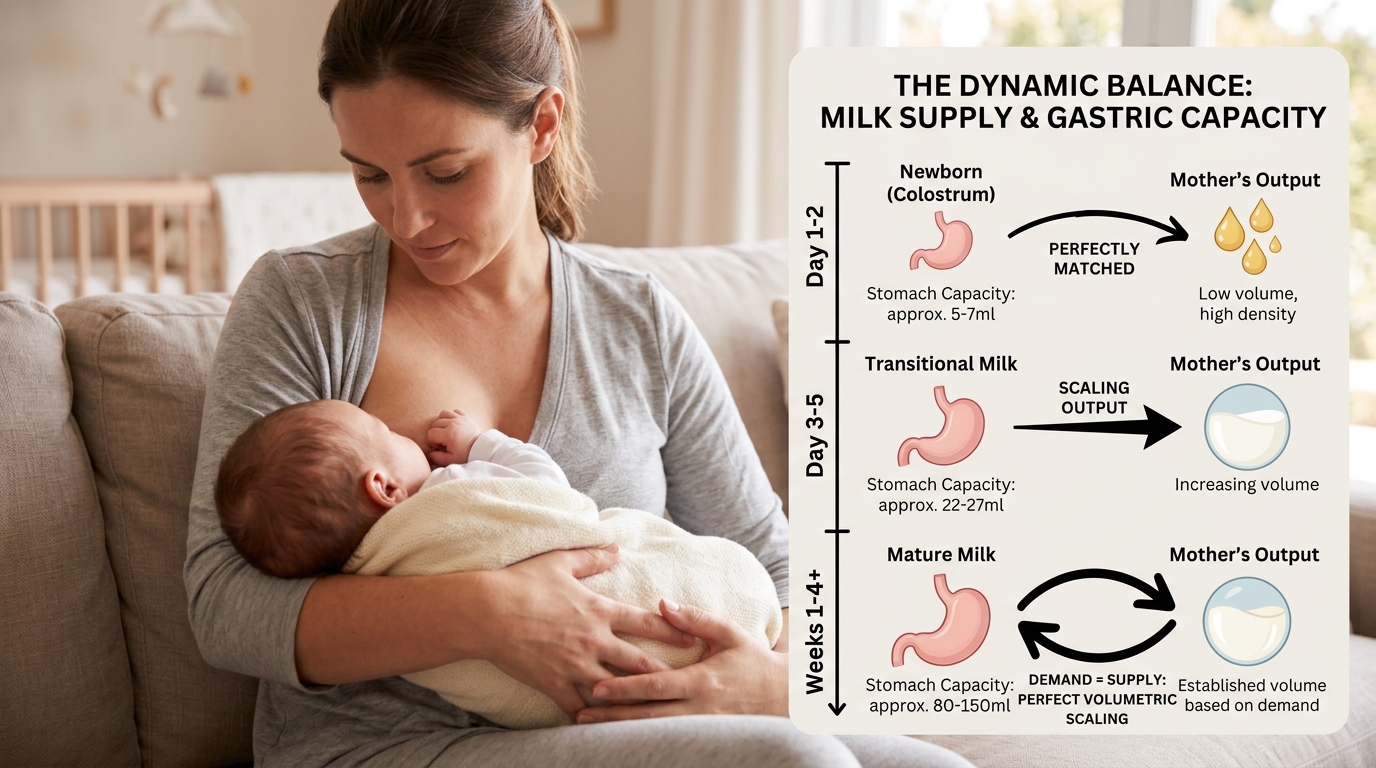
The volumetric output of the human mammary gland scales perfectly and symmetrically with the anatomical capacity and physiological maturation of the infant’s expanding gastrointestinal tract. In the immediate postpartum period, the infant’s stomach capacity is extremely restricted, and the corresponding maternal milk volume is proportionately minute, correctly prioritizing the delivery of dense immunological factors over sheer fluid hydration.
| Infant Age | Average Stomach Capacity | Milk Consumed Per Feed | Target 24-Hour Intake |
|---|---|---|---|
| Day 1 (0-24 hrs) | 5 to 7 mL (Size of a cherry) | 2 to 10 mL | ~1 oz (30 mL) |
| Day 2 to 3 | 22 to 27 mL (Size of a walnut) | 15 to 30 mL | ~8 oz (240 mL) |
| Day 7 | 45 to 60 mL (Size of an apricot) | 30 to 60 mL (1 to 2 oz) | 10 to 20 oz |
| Weeks 2 to 3 | 80 to 150 mL (Size of an egg) | 60 to 90 mL (2 to 3 oz) | 15 to 25 oz |
| 1 to 6 Months | >150 mL | 90 to 120 mL (3 to 4 oz) | 24 to 32 oz |
During the initial 24 to 48 hours of life, exclusively breastfed newborns consume extremely minimal volumes, often just 5 to 10 mL per feed, but do so at exceptionally high frequencies, nursing approximately 8 to 12 times per 24-hour cycle. Because human milk is highly bioavailable and easily digested, gastric emptying is incredibly rapid, leaving the newborn hungry frequently. This continuous high-frequency feeding acts as the critical biological stimulus strictly necessary for the upregulation of prolactin receptors. By the time the infant reaches 1 month of age, mature milk volume stabilizes at a remarkably consistent average of 750 to 800 mL per 24-hour period, a remarkable physiological feat requiring substantial maternal energetic expenditure.
6. The Macronutrient Architecture and Protein Biochemistry
Excluding its water content, which comprises a highly stable 87% to 88% of the total volume, the solid components of mature HBM operate at an osmolarity of approximately 286 mOsm/L and a specific gravity of 1.030. The energy density of human milk is exquisitely calibrated, successfully delivering approximately 20 kcal per ounce (0.67 kcal/cc). The unique caloric distribution of HBM provides 40 percent of its calories from carbohydrates, 50 percent from fats, and a highly controlled, incredibly specific 6 percent from proteins.
The protein concentration of mature HBM ranges from roughly 0.8 to 1.1 g/100 mL. In stark contrast, whole cow milk contains more than triple this amount, providing roughly 3.3 to 3.4 g/100 mL of protein, an overwhelmingly high concentration biologically designed for an ungulate calf that must double its birth weight in roughly 40 days to successfully evade predation. Human Milk heavily exhibits a whey-predominant profile, with a whey-to-casein ratio of roughly 60 to 40. The primary whey protein is α-lactalbumin. The specific casein micelle structures in HBM result in the exact formation of loose, incredibly soft, and highly flocculent curds in the infant’s stomach, allowing for rapid enzymatic degradation. Conversely, bovine milk exhibits a casein-predominant profile (20 to 80), dominated by αS1-casein, which forms large, rubbery, impenetrable curds that severely delay gastric emptying and cause profound gastrointestinal distress in human neonates.
7. Lipid Chemistry and the Significance of sn-2 Palmitate
Lipids represent the absolute most crucial energy vector for the rapidly developing brain, successfully supplying approximately 50 percent of the infant’s total energetic requirements. Mature HBM safely contains 3.5 to 4.5 g/dL of fat, which is heavily concentrated as pure triglycerides. This highly complex lipid matrix is exceptionally rich in essential long-chain polyunsaturated fatty acids (LCPUFAs), such as docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA).
A profound structural distinction exists in the triglyceride architecture of HBM compared to bovine milk and standard vegetable oils. In human milk, the predominant long-chain saturated fatty acid is palmitic acid. Crucially, 70% to 88% of all palmitic acid in HBM is securely esterified at the specific middle position, the sn-2 (or beta) position of the glycerol backbone. Because the palmitic acid is situated at the sn-2 position, it safely remains attached to the glycerol backbone during digestion, forming an sn-2 monoglyceride that is highly soluble and easily absorbed by the intestinal enterocytes. In conventional infant formulas, palmitic acid is frequently esterified at the outer sn-1 and sn-3 positions, releasing free palmitic acid into the gut that binds aggressively with free calcium ions to form highly insoluble calcium soaps, resulting in severe constipation and the dangerous malabsorption of vital dietary calcium.
8. Carbohydrates and the Lactase Imperative
Lactose is the dominant carbohydrate completely present in HBM, successfully maintained at a remarkably stable and high concentration of 67 to 70 g/L in mature milk. Carbohydrates comprise approximately 7 percent of HBM and account for exactly 40 percent of its total caloric reserve. Upon safely reaching the small intestine, lactose is rapidly metabolized by the enzyme lactase, situated perfectly on the brush border of the intestinal epithelium, directly into the monosaccharides glucose and galactose.
These incredibly simple sugars supply the massive, continuous energy demands of the rapidly growing human brain. Furthermore, lactose exerts incredibly high osmotic pressure completely within the mammary gland, actively driving water deeply into the alveoli and perfectly maintaining fluid balance within the milk volume. In the infant gut, the safe fermentation of unabsorbed lactose slightly acidifies the luminal environment, an absolutely essential process that strongly promotes the solubility and subsequent rapid absorption of vital minerals, including critical calcium and phosphorus.
9. The Pathological Hazard of Renal Solute Load
The infant kidney is anatomically and functionally highly immature, entirely unable to safely concentrate urine or effectively clear waste as efficiently as a mature adult kidney. The concept of Renal Solute Load (RSL) refers to the sum total of non-metabolizable dietary components, primarily heavy dietary proteins and complex electrolytes like sodium and potassium, that absolutely must be filtered and safely excreted via the fragile kidneys.
| Nutritional Matrix | Protein (g/100mL) | Pathophysiological Risk to Neonate |
|---|---|---|
| Human Breast Milk | 0.8 to 1.1 | Optimal hydration maintenance; safely within renal limits. |
| Whole Cow Milk | 3.3 to 3.4 | Highly elevated; requires excess water for excretion. |
| Goat Milk | ~3.3 | Extremely elevated (High Cl, K, Na); severe risk of GI bleeding. |
| Skim / 2% Cow Milk | 3.4+ | Dangerously elevated; severe risk of hypernatremic dehydration. |
Feeding a human infant entirely unmodified cow or goat milk strictly prior to 12 months of age is biologically incredibly hazardous and absolutely universally condemned by global health authorities. The massive excessive protein load, securely combined with dangerously high electrolyte levels, produces a totally high volume of toxic nitrogenous waste. To effectively excrete these excess solutes, the neonatal kidney must forcefully draw obligatory water directly from the infant’s delicate tissues and vascular space into the urine, rapidly precipitating deadly hypernatremic dehydration. Because skim milk lacks fat, infants will consume massive volumes to meet caloric needs, resulting in a sodium intake up to 12 times the acceptable physiological limit.
10. Immunoglobulins and Defensive Proteins
Human breast milk operates actively as an incredibly dense vector of passive immunity and an active regulator of infant tissue development. It effectively bridges the highly dangerous immunological gap entirely between the sterile, completely protected environment of the womb and the highly pathogenic external world. The primary humoral antibody completely transferred via HBM is Secretory Immunoglobulin A (sIgA), a whey protein that represents a staggering 80% to 90% of the total immunoglobulins safely present in breast milk.
Originating directly from the maternal gut-associated lymphoid tissue, the dimeric structure of sIgA renders it highly resistant to proteolytic degradation in the infant’s acidic stomach. It survives intact to perfectly coat the mucosal surfaces of the infant’s gastrointestinal tract, binding directly to pathogens and physically blocking their adhesion to epithelial cells. Operating flawlessly in tandem with sIgA is Lactoferrin, a highly potent iron-binding glycoprotein that reaches massive concentrations of up to 7 g/L in colostrum. Lactoferrin tightly sequesters free iron in the gut lumen, completely starving pathogenic Gram-negative bacteria (like E. coli) of the exact resources they severely require for active replication.
11. Exosomes and MicroRNAs: Epigenetic Regulation
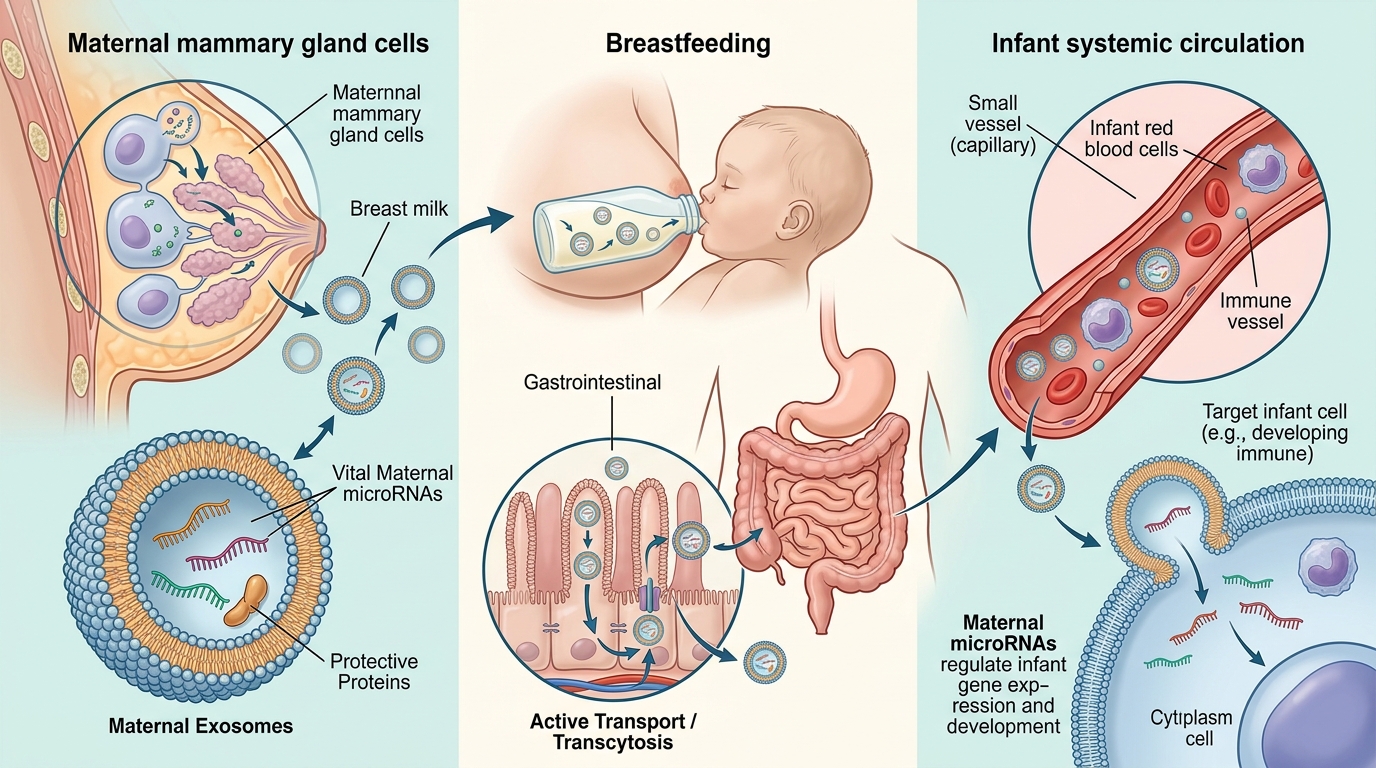
Recent incredible advances in advanced molecular biology have totally uncovered the critical, paradigm-shifting role of perfectly formed HBM-derived exosomes. These are highly advanced nanoscale extracellular vesicles that securely encapsulate and transport a massive payload of bioactive molecules, distinctly including highly complex microRNAs (miRNAs). HBM is remarkably enriched with exactly over 1400 distinct, identifiable miRNAs.
MiRNAs are short, highly complex non-coding RNA sequences that securely regulate gene expression post-transcriptionally by smoothly binding exactly to target messenger RNAs within the infant’s cells, effectively inhibiting their translation into proteins and selectively silencing specific genes. Beautifully protected by the robust, double-lipid bilayer exactly of the exosomes, these vital maternal miRNAs completely survive the harsh acidic degradation of the infant’s gastrointestinal tract. They are actively absorbed deeply into the systemic circulation, where they exert profound epigenetic control over the infant’s physiology, perfectly regulating genes critical entirely for immune system development, stem cell differentiation, and the successful mitigation of future tumor risk.
12. The HAMLET Complex: Tumoricidal Activity
A remarkable, almost unprecedented scientific discovery entirely within the bioactive repertoire of HBM is the highly lethal HAMLET complex (Human Alpha-lactalbumin Made Lethal to Tumor cells). Under normal physiological conditions within the safe mammary gland, the native human whey protein α-lactalbumin strictly coordinates a calcium ion and functions safely as a simple co-enzyme in the synthesis of lactose, possessing absolutely no tumoricidal properties.
However, when native α-lactalbumin is safely ingested by the infant and actively exposed directly to the highly acidic environment of the infant’s stomach, it undergoes a highly crucial structural transformation. The acidic environment causes the protein to partially unfold, releasing its calcium ion to strongly form a calcium-free apo-state. In this conformationally fluid state, the protein becomes highly reactive and firmly binds with oleic acid. The binding of oleic acid permanently stabilizes the protein, successfully generating the active HAMLET complex. HAMLET exhibits highly potent, broad-spectrum tumoricidal activity, explicitly targeting the plasma membranes of rapidly dividing oncologic cells, inducing rapid, irreversible apoptosis (cell death) in the tumor cells while seamlessly leaving completely healthy cells entirely unaffected.
13. Human Milk Oligosaccharides and Genetic Determinism
Human breast milk is uniquely incredibly dense in highly complex, totally indigestible carbohydrates known globally as Human Milk Oligosaccharides (HMOs). Representing the third most abundant solid component exactly in HBM, HMO concentrations average an impressive 12 to 14 g/L in mature milk. Because HMOs are virtually entirely indigestible perfectly by the infant’s endogenous digestive enzymes, they serve a strictly critical evolutionary purpose: they are highly potent, selective prebiotics.
The total composition, massive diversity, and exact concentration of HMOs in any given mother’s milk are absolutely not uniform; they are strictly governed directly by the mother’s inherent genetic profile, specifically the complex interplay of the FUT2 (Secretor) and FUT3 (Lewis) genes. The FUT2 gene encodes the α-1,2-fucosyltransferase enzyme. Mothers possessing an active FUT2 gene are phenotypically termed Secretors, and their milk is massively enriched with 2′-fucosyllactose (2′-FL), which can account for nearly 30 percent of all HMOs. Mothers with a nonsense mutation in this gene are Non-secretors, and their milk is completely devoid of 2′-FL. Because the highly specific molecular structures of HMOs totally dictate exactly which bacterial strains (like Bifidobacterium infantis) can safely thrive in the gut, the precise composition of the infant’s founding microbiome is directly downstream exactly of the mother’s genetic secretor status.
| Phenotype Classification | FUT2 Status | FUT3 Status | 2′-FL Presence |
|---|---|---|---|
| Secretor, Lewis-positive | Active | Active | Abundant |
| Non-secretor, Lewis-positive | Inactive | Active | Absent |
| Secretor, Lewis-negative | Active | Inactive | Abundant |
| Non-secretor, Lewis-negative | Inactive | Inactive | Absent |
14. The Breast Milk Microbiome and Retrograde Feedback
Historically, modern medical science erroneously considered human breast milk to be a completely sterile fluid. Modern next-generation sequencing techniques have unequivocally completely dispelled this inaccurate notion, brilliantly revealing a highly complex, native HBM bacteriome that acts explicitly as a continuous source of highly commensal microbial inoculant for the fragile infant gut. This incredible core is universally dominated seamlessly by beneficial lactic acid bacteria heavily including Lactobacillus and Bifidobacterium. Maternal dendritic cells actively sample commensal bacteria exactly from the maternal gut lumen and precisely deliver them alive directly to the mammary gland for total inclusion completely in the milk.
Crucially, the complex interaction between the maternal mammary gland and the nursing infant is absolutely not a simple unidirectional flow of liquid nutrients; it securely constitutes a highly dynamic, bidirectional immunological dialogue. During active breastfeeding, the physical vacuum created perfectly by the infant’s intra-oral pressure safely induces a profound physiological phenomenon known exactly as retrograde duct flow. Small volumes of the infant’s saliva are safely drawn backward directly into the maternal milk ducts. If the infant is experiencing an active infection, their saliva contains unique viral or bacterial antigens. The maternal mammary gland instantly detects these foreign antigens and rapidly upregulates the heavy synthesis of targeted macrophages and highly specific sIgA antibodies, safely delivering an elevated, custom-synthesized payload of immunological factors directly back to the infant in highly subsequent feedings.
15. Cellular Transfer and Pluripotent Stem Cells
Beyond its vast array of totally biochemical and strictly microbial components, HBM brilliantly contains a highly robust, totally living cellular population. Recent incredible technologic advances have explicitly resulted precisely in a massive breakthrough discovery: the verified presence exactly of living, pluripotent-like stem cells directly in human breast milk. These human breast milk stem cells (hBmSCs) reliably exhibit remarkable biological properties, securely expressing classical markers of pluripotency, specifically OCT4 and NANOG, fully capable exactly of safely differentiating directly into completely distinct cells of all three germ layers.
During the incredibly normal course of daily breastfeeding, the fragile infant seamlessly ingests literally millions of these vital maternal stem cells entirely daily. Because the infant’s gastric acid profile is significantly less robust, these highly unique maternal cells actively transmigrate directly across the delicate intestinal epithelium and safely enter the infant’s highly systemic bloodstream. They successfully migrate directly to, and engraft deeply perfectly within, multiple solid organs, specifically heavily within the central nervous system. This phenomenon is known flawlessly as fetomaternal microchimerism, completely explaining why individuals who were breastfed demonstrate a significantly highly improved acceptance rate entirely for maternal organ transplants later in life.
16. Chrononutrition and Circadian Rhythms
The exact composition of HBM is absolutely not a highly static, unchanging formula; rather, it beautifully exhibits highly synchronized, extremely vital circadian oscillations, actively changing dramatically across a rigorous 24-hour period. The intensive study exactly of how the precise timing of nutritional intake influences deep physiological rhythms is globally termed chrononutrition. Postnatally, the infant’s endogenous circadian rhythms are highly immature and disorganized. HBM smoothly serves exactly as the incredibly critical exogenous synchronizer, safely delivering temporally specific neuroendocrine signals to seamlessly entrain the infant’s biological clock.
Milk produced specifically during active daylight hours flawlessly exhibits significantly heavily elevated concentrations of cortisol, actively promoting alertness and metabolic activation. Conversely, exactly as daylight strictly fades, cortisol drops precipitously, and the exact concentration of melatonin in the milk rises, strongly peaking deeply during the dark night hours. Night milk contains disproportionately highly elevated levels exactly of tryptophan, the direct biochemical precursor to safely producing serotonin and endogenous melatonin. This continuous, highly specific time-of-day signaling securely helps infants rapidly consolidate their sleep architecture. Feeding an infant morning-pumped, entirely cortisol-rich milk exactly at midnight can inadvertently severely deliver completely discordant biological signals, dangerously disrupting their developing sleep architecture.
17. Donor Milk Banking and Pasteurization Dynamics

For highly vulnerable, critically ill premature infants securely residing perfectly within neonatal intensive care units (NICUs) who totally absolutely cannot seamlessly access their own mother’s specific milk, the global medical community heavily relies entirely upon formally established Donor Human Milk Banks. These highly sterile, rigorously regulated facilities collect, thoroughly screen, actively process, and safely dispense donated HBM exactly to prevent highly devastating, entirely deadly intestinal morbidities, most specifically the catastrophic disease necrotizing enterocolitis (NEC).
To explicitly absolutely guarantee total microbiological safety and entirely definitively eliminate the risk of totally transmitting extremely dangerous viral pathogens precisely such as HIV or Cytomegalovirus (CMV), completely all pooled donor milk absolutely must undergo incredibly rigorous thermal processing, universally executed via Holder Pasteurization. The strict Holder method mathematically requires the precise, completely sustained heating exactly of the pooled milk accurately to exactly 62.5 °C for exactly 30 minutes, seamlessly followed rapidly by aggressive flash cooling. While this exact thermal intervention flawlessly totally ensures complete microbiological sterility, the intense heat sadly unavoidably denatures and entirely degrades incredibly specific, highly fragile bioactive components. The specific process destroys entirely all living leukocytes and vital stem cells, reduces incredibly critical sIgA concentrations significantly by exactly roughly 20 to 30 percent, and completely totally absolutely irreversibly obliterates the highly sensitive Bile Salt-Stimulated Lipase (BSSL), entirely forcing the fragile premature infant to fully completely totally rely absolutely heavily on their incredibly own highly immature endogenous pancreatic lipases perfectly to safely completely digest the totally exact complex milk lipids.



